CAR-T Cell Therapy: Redesigning the Immune System to Fight Cancer
2025-12-03
CAR-T Cell Therapy: Redesigning the Immune System to Fight Cancer
A New Option for Patients with Refractory Blood Cancers
“There are no remaining standard treatment options.”
For patients with refractory blood cancers who have not responded to chemotherapy, radiation therapy, or bone marrow transplantation, CAR-T cell therapy offers a new line of hope.
Since its first FDA approval in 2017, CAR-T therapy has shown meaningful response rates in specific groups of patients with hematologic malignancies.
At the same time, it comes with important considerations — high cost (often exceeding 100 million KRW, roughly $70,000–$80,000), the need for careful management of side effects, and a complex manufacturing process.
What exactly is CAR-T cell therapy? Which patients are eligible, and what are its current outcomes and future potential?
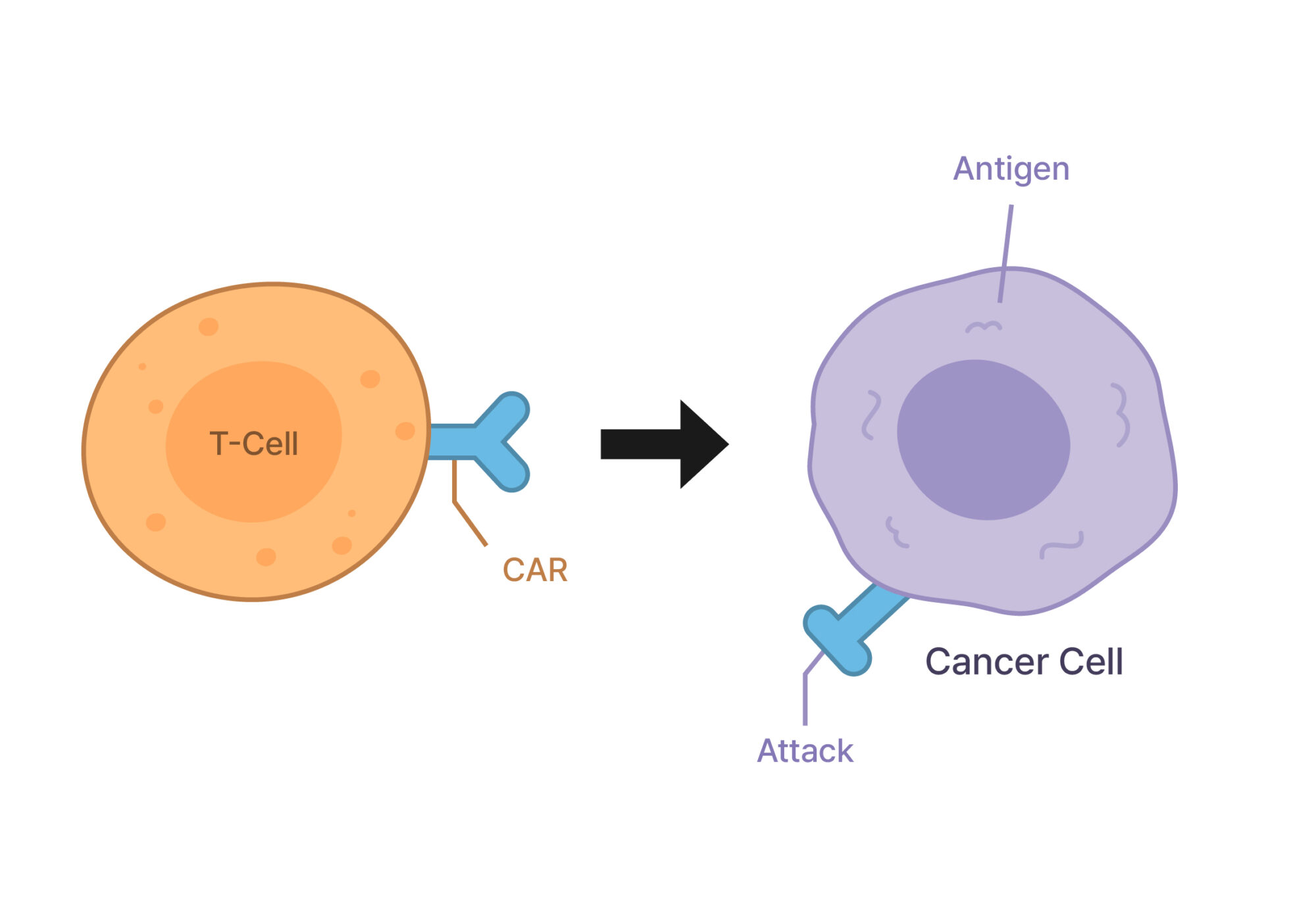
Figure 1. Mechanism of CAR-T Cell Therapy CAR-T cells recognize and bind to specific antigens on the surface of cancer cells through their chimeric antigen receptors (CARs), leading to targeted destruction of the cancer cells.
What Is CAR-T Therapy? Precision Medicine That “Redesigns” the Immune System
Why Our Immune System Fails to Detect Cancer
T cells are the key soldiers of our immune system. Their main mission is to identify and eliminate virus-infected or abnormal cells.
However, cancer cells are cunning — they use various “camouflage” strategies to escape immune surveillance:
Immune checkpoint activation : Sending false signals that say, “I’m a normal cell.”
Reduced antigen expression: Hiding surface markers that T cells would normally recognize.
Creating an immunosuppressive microenvironment : Forming a protective barrier around the tumor to block immune attacks.
As a result, our T cells often either fail to recognize the presence of cancer cells or, even when they do, cannot effectively attack them.
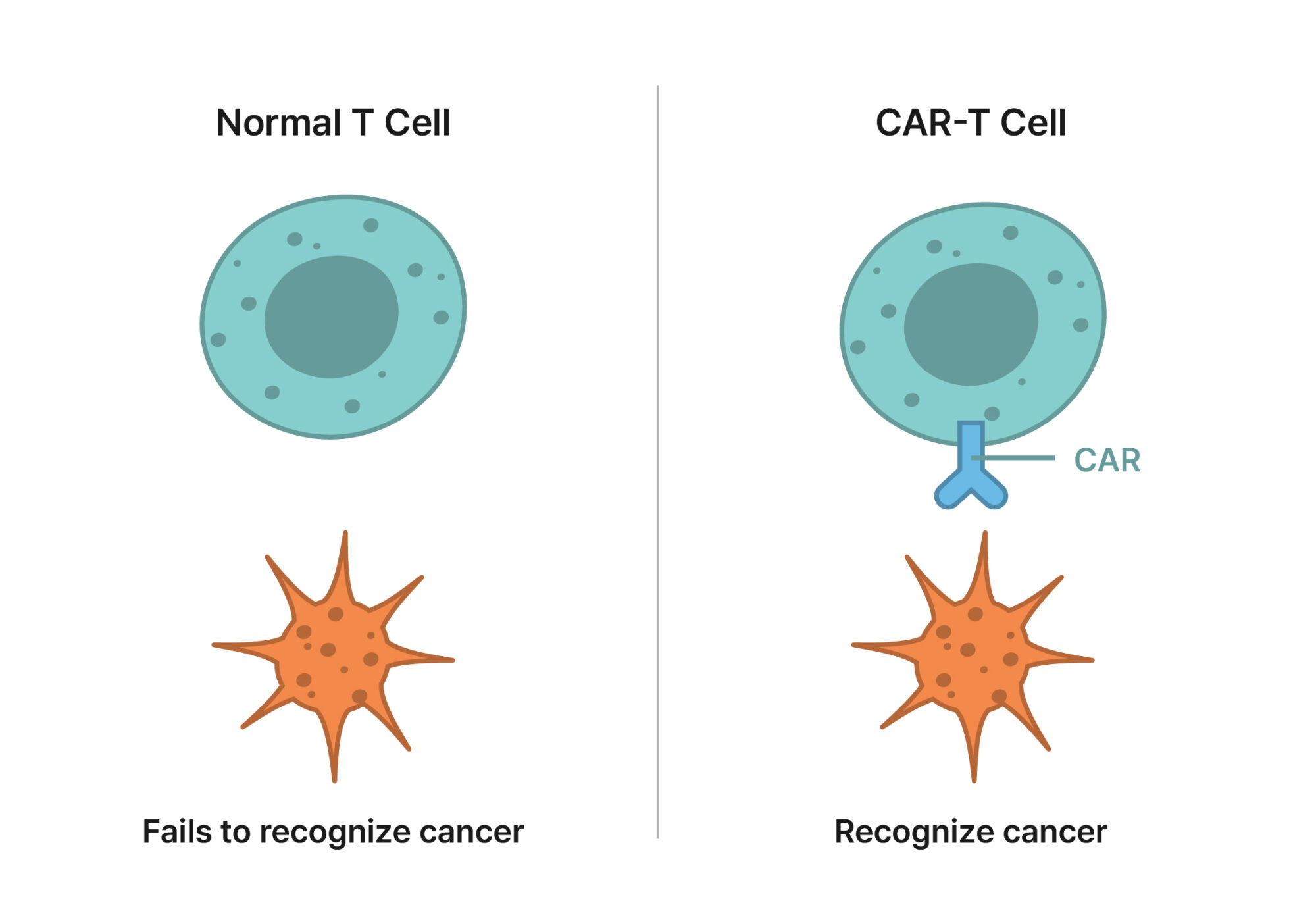
Figure 2. Comparison Between Normal T Cells and CAR-T Cells
Normal T cells cannot recognize cancer cells, whereas CAR-T cells—equipped with chimeric antigen receptors (CARs)—can specifically identify antigens on the surface of cancer cells.
CAR-T: Equipping T Cells with GPS and Weapons
CAR-T (Chimeric Antigen Receptor T-cell) therapy directly tackles this challenge.
It involves extracting a patient’s own T cells, genetically reprogramming them to enhance their cancer-fighting ability, and reinfusing them back into the patient.
The process works as follows:
T cell collection : Blood is drawn from the patient using leukapheresis to harvest T cells.
Genetic engineering : In the lab, T cells are modified to express a chimeric antigen receptor (CAR)—a special “radar” that recognizes cancer-specific antigens.
Cell expansion : The engineered T cells are multiplied into hundreds of millions of cells (a process that takes about two weeks).
Reinfusion : These reprogrammed T cells are then infused back into the patient, where they seek out and destroy cancer cells.
In vivo persistence: Once inside the body, CAR-T cells continue to proliferate, providing long-lasting immune surveillance and potential remission.
The most groundbreaking aspect of this therapy is that CAR-T cells are “living drugs.” Unlike conventional chemotherapy, which uses external chemical agents, CAR-T therapy turns a patient’s own immune cells into active cancer-fighting agents within the body.
CAR-T Therapy in Practice: What the Data Tell Us
Response Rates in Blood Cancers
Currently, FDA-approved CAR-T therapies are mainly used to treat relapsed or refractory hematologic malignancies — that is, when standard chemotherapy, radiation, or transplantation have already failed.
Acute Lymphoblastic Leukemia (ALL) — Pediatric and Young Adult
Severe: Seizures, loss of consciousness, cerebral edema.
Prolonged Cytopenia
Extended low blood counts may increase infection risk.
Why CAR-T Therapy Is So Expensive: The Complexity of Manufacturing
The Challenge of Personalized Production
Unlike conventional drugs that can be mass-produced in factories, each CAR-T product must be custom-made for a single patient. This individualized process makes manufacturing both time-consuming and costly.
The 5-Step CAR-T Manufacturing Process
Step 1. Leukapheresis ( ≈ 1 day )
White blood cells are separated from the patient’s blood (only ~2 % of total blood volume).
This specialized procedure takes about 3 – 4 hours.
Step 2. T-Cell Isolation and Activation ( 2 – 3 days )
T cells are extracted from the white blood cell fraction.
Growth factors “wake up” dormant T cells and prepare them for engineering.
Cell quality can vary depending on the patient’s condition.
Step 3. Genetic Engineering ( ≈ 1 day )
A viral vector is used to insert the CAR (chimeric antigen receptor) gene into T cells.
This is one of the most delicate and critical steps.
Each batch must be validated for gene-insertion efficiency and safety.
Step 4. Cell Expansion ( 7 – 14 days )
The engineered T cells are expanded from millions to billions.
Continuous 24-hour monitoring is required.
Growth rate and cell viability are closely tracked.
Step 5. Quality Control and Cryopreservation ( 2 – 3 days )
The final product is tested for cell count, purity, contamination, and potency.
The cells are then preserved at –196 °C in liquid nitrogen until infusion.
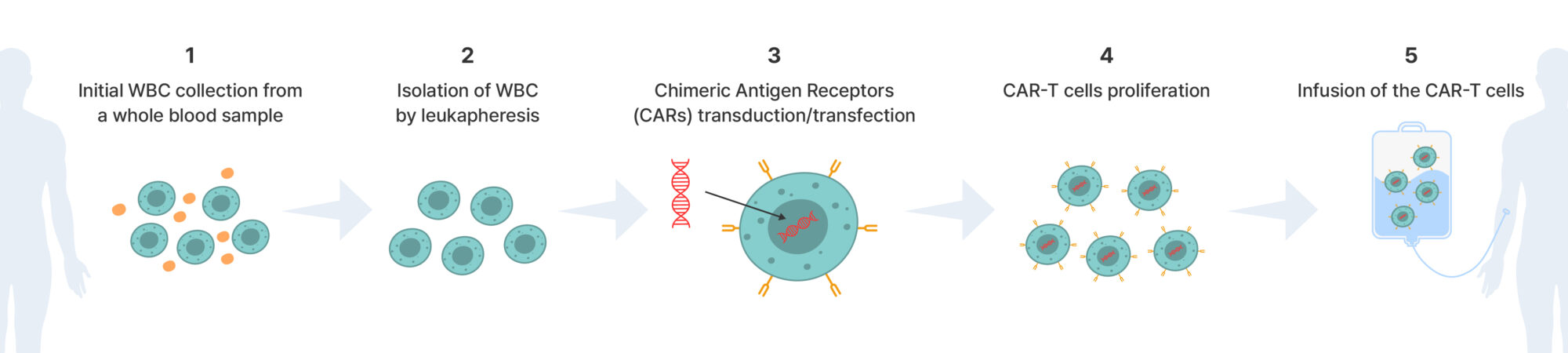
Figure 3. How CAR-T Therapy Is Made — From Patient’s Cells to Living Medicine
Quality Control: The Factor That Determines Success or Failure
The most critical element in CAR-T manufacturing is precise quality control (QC). At every stage of production, several key parameters must be monitored:
Viability: proportion of living cells — must exceed 70 %
Purity: removal of unwanted cells or contaminants
Potency: measurement of CAR expression and tumor-killing ability
Traditional manual cell-counting methods are time-consuming (5 – 10 minutes per sample), prone to operator error (10 – 20 % coefficient of variation), and often lack reproducibility.
To overcome these limitations, automated cell-counting systems have become essential.
For example, instruments such as LUNA-FX7™ (Logos Biosystems) provide:
< 1 % coefficient of variation for superior precision
Simultaneous analysis of up to 8 samples, improving throughput
Compliance with 21 CFR Part 11 regulatory standards
Real-time monitoring of cell growth and productivity
By integrating such automation technologies, CAR-T manufacturers can ensure consistent product quality across batches and maintain the high reproducibility and traceability required for patient safety.
The Future of CAR-T Therapy: How Far Can It Go?
The Challenge of Solid Tumors
The biggest frontier for CAR-T therapy is treating solid tumors — such as lung, colon, pancreatic, and breast cancers — where CAR-T has not yet matched its success in blood cancers.
Why solid tumors are difficult:
Limited infiltration : T cells have trouble penetrating the dense tumor mass.
Immunosuppressive microenvironment : Tumors create conditions that block immune activity.
Antigen heterogeneity : Each cancer cell may express different antigens, making it hard to find a universal target.
Off-target risk: Some tumor antigens are also found on healthy cells, raising the risk of side effects.
Research directions:
Multi-target CAR-T : Designed to recognize multiple tumor antigens simultaneously.
Armored CAR-T : Engineered to resist or neutralize immunosuppressive signals in the tumor environment.
Localized delivery : Injecting CAR-T cells directly into tumor sites to enhance precision and safety.
Allogeneic CAR-T: The “Off-the-Shelf” Vision
Currently, most CAR-T therapies are autologous — made from a patient’s own cells. Researchers are now developing allogeneic (donor-derived) CAR-T therapies that can be pre-manufactured and stored for immediate use.
Advantages of allogeneic CAR-T:
Immediate availability — no need to wait for individual cell processing.
Reduced cost through large-scale production (potentially one-fifth the cost).
Consistent quality due to standardized manufacturing.
Challenges to overcome:
Graft-versus-host disease (GVHD) : Donor cells may attack the patient’s tissues.
Immune rejection : The patient’s immune system may eliminate donor-derived CAR-T cells.
The Rise of Next-Generation Immune Cell Therapies
Beyond CAR-T, new engineered immune-cell therapies are emerging that may address its limitations.
Safer than T cells (lower risk of cytokine storm).
Can be used allogeneically (from healthy donors).
May show stronger potential against solid tumors.
TCR-T (T Cell Receptor) Therapy
Recognizes intracellular antigens via MHC presentation.
Expands the range of targetable cancers beyond surface proteins.
TIL (Tumor-Infiltrating Lymphocyte) Therapy
Uses immune cells that have already infiltrated the tumor.
Especially promising for solid tumors, including melanoma.
The Fusion of AI and Biomanufacturing
The integration of artificial intelligence (AI) and automation is transforming how CAR-T therapies are produced.
Emerging technologies:
AI-based quality prediction : Early data can forecast the final product’s potency.
Real-time process optimization : Automated systems adjust culture conditions based on live cell-growth analytics.
Fully automated production : Robotics enable closed, contamination-free manufacturing.
Digital twins : Virtual simulation models reduce process failure and enhance consistency.
Conclusion: A Powerful Yet Imperfect Therapy
CAR-T cell therapy offers a meaningful treatment option for patients with relapsed or refractory blood cancers who have exhausted conventional therapies. In some cases, it has achieved durable long-term remission, providing new hope where few options remain.
However, several key considerations must be kept in mind:
Not all patients respond — approximately 20–30% show no initial effect.
High cost and limited accessibility, despite gradual improvement with insurance coverage.
Severe side effects such as cytokine release syndrome (CRS) and neurotoxicity require close monitoring by experienced specialists.
Limited efficacy in solid tumors, as current approvals are restricted mainly to blood cancers.
Over the next decade, advancements in allogeneic CAR-T, solid tumor targeting, and cost reduction are expected to further expand the potential of this therapy. For now, however, CAR-T remains a highly personalized treatment reserved for patients who meet strict eligibility criteria and are managed under expert medical supervision.
CAR-T therapy can be life-extending for selected patients, but it is not a universal solution. Treatment decisions should always be made in close consultation with qualified healthcare professionals.
REFERENCES
1 Park JH, Rivière I, Gonen M, et al. Long-Term Follow-up of CD19 CAR Therapy in Acute Lymphoblastic Leukemia. N Engl J Med. 2018;378(5):449-459. doi:10.1056/NEJMoa1709919
2 Maude SL, Laetsch TW, Buechner J, et al. Tisagenlecleucel in Children and Young Adults with B-Cell Lymphoblastic Leukemia. N Engl J Med. 2018;378(5):439-448.
3 Neelapu SS, Locke FL, Bartlett NL, et al. Five-year follow-up of ZUMA-1 supports the curative potential of axicabtagene ciloleucel in refractory large B-cell lymphoma. Blood. 2023;141(19):2307-2315. doi:10.1182/blood.2022018893
4 Locke FL, Ghobadi A, Jacobson CA, et al. Long-term safety and activity of axicabtagene ciloleucel in refractory large B-cell lymphoma (ZUMA-1): a single-arm, multicentre, phase 1-2 trial. Lancet Oncol. 2019;20(1):31-42.
5 Pereira R, Bergantim R. An Assessment of the Effectiveness and Safety of Chimeric Antigen Receptor T-Cell Therapy in Multiple Myeloma Patients with Relapsed or Refractory Disease: A Systematic Review and Meta-Analysis. Int J Mol Sci. 2024;25(9):4996. doi:10.3390/ijms25094996
Logos Biosystems provides a diverse portfolio of automated cell counters designed to meet various laboratory requirements. To learn more, visit www.logosbio.com.